Case of the Month November 2011
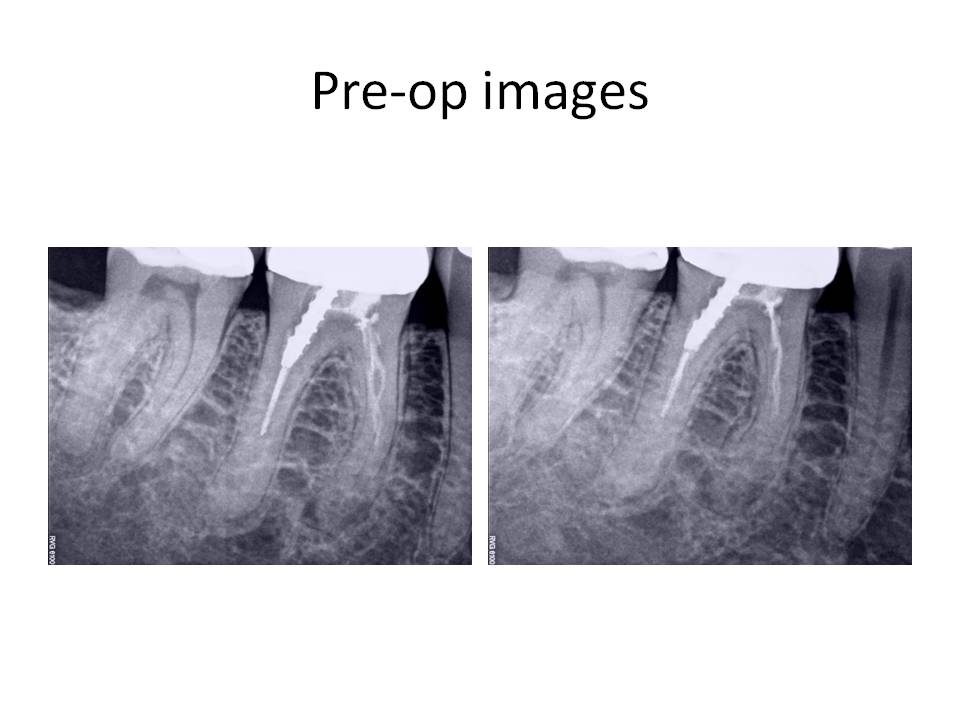
The clinical diagnosis is Previously treated #30 with asymptomatic periapical periodontitis.
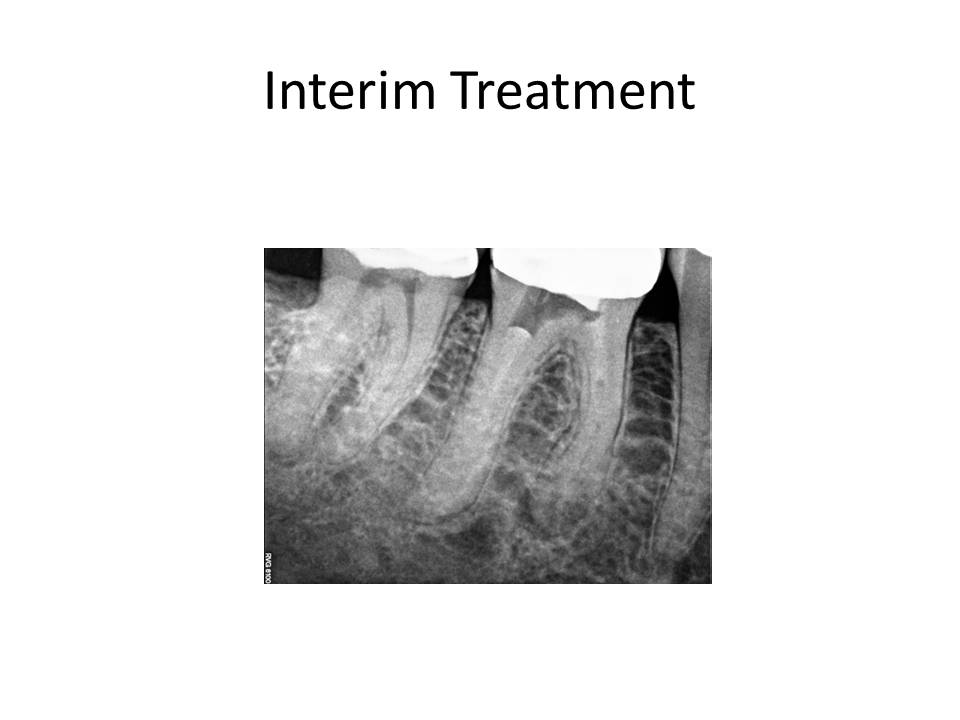
Retreatment of the root canal was recommended and the patient decided to proceed with the treatment. The problems that are anticipated when the case is viewed radiographically are as follows: Preservation of the crn (if possible), removal of the threaded post in the distal root, removal of the carrier-based obturation in the distal root, negotiating the meisal canals after removal of the existing gutta-percha. The mesial canals appear to have been ledged during the previous treatment and this always poses a significant challenge. Careful exploration of the canals with pre-bent small files and a gentle touch is what is needed in these situations. At the initial visit, the tooth was accessed, the threaded post was removed with an ultrasonic and copious water to prevent as much heat transfer to the root as possible. The carrier was removed (Soft-core) from the distal root and this canal was negotiated to the apex. The mesial canals presented with a more difficult challenge to negotiation. The canals were severly ledged and also joined, as evidenced by the drying of one canal led to the other canal being dried as well. I was unable to complete the case in the first appointment. Calcium hydroxide was placed and the patient was reappointed. The interim radiograph is as follows:
At the second appointment, the patient was asymptomatic, the tooth was again accessed and the process of trying to negotiate the mesial canals was ensued. I think I went through approximately 50 hand files in trying to gain patency. Being persistent paid off and I was finally able to gain access to the apex. The case was cleaned and shaped, and obturated with warm gutta-percha. The completed case is as follows: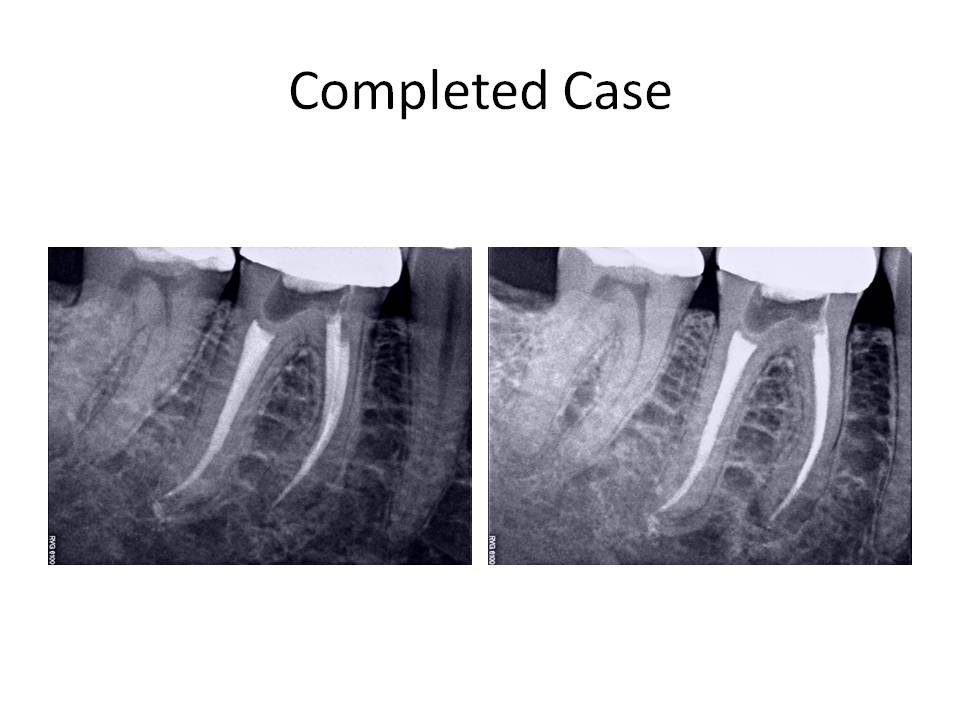
This case demonstrated a challenge to canal negotiation. Proper technique and an understanding of my goals was essential in order to properly treat the case. Certainly, I could have initally opted for a root end resection. However, I felt fairly confident that I could manage the retreatment without having to go to an apicoectomy. I welcome any comments or feedback regarding this case. Thank you again for entrusting my office with the care of your valued patients.